
New York University Uses NHLBI Program for Filipino American Heart Health
Overview
Heart disease is one of the leading causes of death across Asian American groups. Filipino Americans—the second-largest Asian American community—have some of the highest rates of obesity and of being overweight, both of which increase their risk for heart disease and high blood pressure.1
The New York University (NYU) Center for the Study of Asian American Health conducted focus groups with Filipino American residents to better understand why Filipino Americans are at a higher risk. Community members who participated expressed concern about heart disease and stroke and said that they did not maintain healthy eating habits or engage in regular physical activity. Residents also reported that they did not have regular access to health care.2
In response to the heart health needs of Filipino American residents, NYU began a partnership with the NHLBI and, in 2005, participated in a strategy development workshop called the Pearls of Wisdom workshop; the school then worked with experts at the NHLBI to help adapt the Honoring the Gift of Heart Health manual to meet the needs of Filipino American communities. NYU provided content review and conducted focus groups and pilot testing as the manual was being created.
In 2007, the NHLBI released Healthy Heart, Healthy Family (HHHF), a set of tools that include a community health worker (CHW) manual, picture cards, handouts, and other materials to help reduce health disparities among Filipino Americans.
Implementation Strategies
Staff from the NHLBI conducted a train-the-trainer workshop to coach the NYU team on how to implement and evaluate the HHHF curriculum. The curriculum has since been used by Project AsPIRE CHWs to provide participants with the knowledge and tools to live healthier lifestyles. Project AsPIRE’s main aim is to implement and assess the efficacy of a CHW intervention to improve hypertension management and access to care among Filipino Americans living in the New York/New Jersey area. NYU has also used the NHLBI’s community education strategy to adapt and use HHHF in their area.
Project AsPIRE screened 829 Filipino Americans and enrolled 237 participants between the ages of 25 and 75 who had either treated or untreated high blood pressure in a randomized control trial intervention. Project staff randomly enrolled each participant in one of two groups. The treatment arm group (n=113) was educated using the HHHF curriculum and received four one-on-one follow-ups with CHWs and at least one follow-up phone call each month from the CHW. The control group (n=124) received one-on-one hypertension management education sessions.
After hiring and training four CHWs, NYU staff partnered with businesses and faith-based organizations to run group and one-on-one education sessions. Although the HHHF curriculum was designed to include 10 sessions, when the NYU team noticed that program participants were often unable to attend more than a few sessions, the NYU modified the curriculum to 4 sessions, each 2 hours long, followed by a review and graduation session. CHWs running the NYU program also tied HHHF messages to Filipino American history and culture to help participants relate to the materials. Each class focused on specific topics tied to heart disease.
To further increase participation, the team linked education sessions with physical activity classes, such as yoga or martial arts. Program participants were also offered incentives such as subway cards and discounted memberships to a local gym.
In addition to the program information and activities, group discussions were a large part of each HHHF session. Participants talked about personal challenges with diet, physical activity, and chronic disease management. This type of peer support was similar to other NHLBI CHW programs that foster group discussion around heart health to help participants make important individual and family behavior changes in everyday life.
Key Results/Outcomes
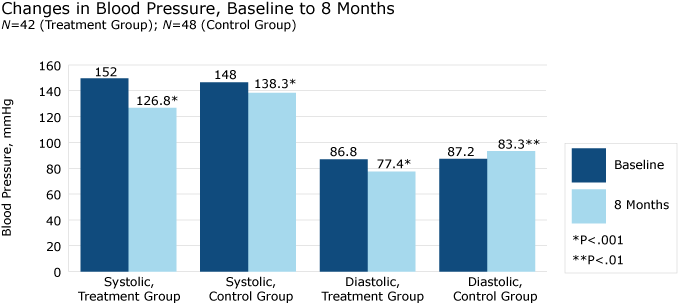
Analyses were performed on 42 treatment participants and 48 control participants who had completed 4-month and 8-month follow-up surveys as of October 2012. Both treatment and control group participants saw reductions in systolic and diastolic blood pressure (BP) at 8 months.
In the treatment group, mean systolic BP decreased from 152.0 mmHG at baseline to 126.8 mmHG at 8 months (P<.001), and mean diastolic BP decreased from 86.8 mmHG at baseline to 77.4 mmHG at 8 months (P<.001). In the control group, mean systolic BP decreased from 148.0 mmHG at baseline to 138.3 mmHG at 8 months (P<.001), and mean diastolic BP decreased from 87.2 mmHG at baseline to 83.3 mmHG at 8 months (P<.01).
Changes in BP were significantly greater in the treatment group than in the control group.
| Blood Pressure | Treatment Group, Baseline | Treatment Group, 8 Months | Control Group, Baseline | Control Group, 8 Months |
|---|---|---|---|---|
| Systolic | 152 | 126.8 (P<.001) | 148 | 138.3 (P<.001) |
| Diastolic | 86.8 | 77.4 (P<.001) | 87.2 | 83.3 (P<.01) |
At 8 months, treatment group participants had a mean change in systolic BP of -25.2 mmHg, while control group participants had a mean change in systolic BP of -9.7 mmHg (P<.001); treatment group participants had a mean change in diastolic BP of -9.4 mmHg, while control group participants had a mean change in diastolic BP of -3.9 mmHg (P<.05). Treatment group participants were also more likely to exhibit controlled BP at 8 months (88.1%) than the control group (54.1%; P<.001).
| Blood Pressure | Treatment Group | Control Group | P Value |
|---|---|---|---|
| Systolic BP | -25.2 | -9.7 | .001 |
| Diastolic BP | -9.4 | -3.9 | .05 |
| Blood Pressure | Treatment Group | Control Group | P Value |
|---|---|---|---|
| Percent with Controlled HBP | 88.1 | -54.1 | .001 |
NYU’s successful experience with HHHF is leading to changes in current program materials. The HHHF manual is being revised to better meet CHWs’ teaching needs and to make the information more accessible for program participants. NYU is looking for ways to reach more people in Filipino American communities with the HHHF manual.
Success Factors
- The HHHF curriculum has been well received by the Filipino American community, due to the fact that the curriculum was culturally tailored for Filipino Americans.
- Project AsPIRE has been able to leverage resources and partnership opportunities between the Center for the Study of Asian American Health and the Kalusugan Coalition, Inc., a community-based organization serving the health needs of the Filipino American community in New York and New Jersey.
- CHWs have played a key part in implementing train-the-trainer, community education, and lifestyle and clinical management outreach activities.
1 Tseng, W., McDonnell, D. D., Takahashi L., Ho, W., Lee, C., & Wong, S. (2010). Ethnic Health Assessment for Asian Americans, Native Hawaiians, and Pacific Islanders [Fact sheet].
[Fact sheet].
2 New York University Center for the Study of Asian American Health. (2007). Community Health Needs & Resource Assessment: An Exploratory Study of Filipino Americans in the New York Metropolitan Area.
Last Updated: June 2014




